
Introduction
Anterior cruciate ligament (ACL) injury is a serious condition that can potentially end an athlete’s career. It often requires surgical reconstruction and a thorough rehabilitation program. The complexity of ACL rehabilitation lies in the need to restore knee stability,
strength, and functional performance to at least pre-injury levels while minimizing the risk of re-injury. While plyometric training (PT) is widely recognized for its benefits in
enhancing athletic performance (Davies et al., 2015), its application in ACL
rehabilitation is frequently overlooked or superficially understood (Buckthorpe & della
Villa, 2021). This literature review aims to highlight the role of PT in ACL rehabilitation,
its underutilization despite evidence-based guidelines recommending its use (Kotsifaki
et al., 2023), and provide practical advice for strength and conditioning coaches and
physiotherapists.
Complexity of ACL Rehabilitation
ACL rehabilitation is a multifaceted process that requires a systematic approach to address
various physiological, functional and psychological deficits post-surgery. The
rehabilitation protocol typically progresses through several stages, beginning with the
immediate post-operative phase, focusing on pain management, swelling reduction,
and regaining knee range of motion. This is followed by phases emphasizing muscle
activation, strength development, neuromuscular control, and functional training
(Buckthorpe et al., 2019b, 2019a). The ultimate goal is to prepare the athlete for a safe
and effective return to sport (RTS), which involves high-level motor skills, agility, and
power.
Guidelines for Plyometric Training in ACL Rehabilitation
Evidence-based guidelines, such as those provided by the Aspetar clinical practice (Kotsifaki
et al., 2023), recommend the inclusion of plyometric exercises in the later stages of
ACL rehabilitation to enhance neuromuscular performance and movement quality
(Buckthorpe, 2019). Plyometric exercises, which involve explosive movements utilizing
the stretch-shortening cycle, are crucial for developing power, coordination and
tendon stifness, all of which are essential for RTS (Herrington et al., 2013). Despite
these recommendations, PT is often underutilized in ACL rehabilitation programs.
Plyometric Training: Benefits and Applications
Plyometric training is a well-established method for improving various aspects of athletic
performance, including strength, speed, and agility. The key benefits of plyometric
training include:
- Enhanced Muscle Power: Plyometric exercises significantly increase muscle power by
improving the efficiency of the stretch-shortening cycle, leading to greater force
production in a shorter period (Davies et al., 2015). - Improved Neuromuscular Coordination: The rapid and dynamic nature of plyometric
exercises enhances neuromuscular control, which is critical for maintaining
joint stability and preventing injuries (Buckthorpe & Villa, 2020). - Increased Tendon Stiffness: Plyometric training increases tendon stiffness, which
contributes to better force transmission and improved athletic performance
(Bleakley & Ne:erström-Wedin, 2023). - Enhanced Proprioception: The proprioceptive demands of plyometric exercises improve
the body’s ability to sense and react to changes in position, which is vital for
dynamic sports movements (Buckthorpe, 2019). - Injury risk reduction: Plyometric training appears to be effective in preventing anterior
cruciate ligament (ACL) injuries. Although there is some conflicting evidence, a
recent trial demonstrated that plyometric training may be more effective than
traditional resistance training in inducing biomechanical changes at the knee
that are associated with a reduced risk of ACL injury (Bocheng et al., 2024)
Plyometric Training in Rehabilitation
First of all, let’s clarify that high intensity plyometric training is safe: no increase in chemical
mediators have been found in ACL reconstructed patients following an 8 week high
intensity plyometric training in respect to low intensity plyometric training
(Chmielewski et al., 2016).
In the context of ACL rehabilitation, plyometric training can address several key objectives:
- Restoring Explosive Strength and Power: ACL injuries often result in significant losses in
muscle strength and power. Plyometric exercises help restore these attributes
by targeting both concentric and eccentric muscle actions (Davies et al., 2015) - Improving Movement Quality: Proper execution of plyometric exercises requires precise
movement patterns, which can help correct compensatory mechanisms
developed post-injury (Buckthorpe & Villa, 2020). - Reducing Re-injury Risk: By enhancing neuromuscular control and proprioception,
plyometric training can reduce the likelihood of re-injury during high-demand
activities (Buckthorpe & della Villa, 2021). - Combination with eccentric traing: A combined eccentric and plyometric training
protocol proved to be the most effective approach for enhancing both stability
and functional performance (Kasmi et al., 2021).

Practical Recommendations & Program Design
Designing an effective PT program for ACL rehabilitation involves several key considerations:
- Progressive Overload: Start with low-intensity exercises and gradually increase the
intensity and complexity as the athlete demonstrates improved strength and
control or regress if there is any sign of increased pain or swelling. Early-stage exercises may
include bilateral jumps and hops, progressing to unilateral and multi-directional
movements (Buckthorpe et al., 2019a, 2019b). - Volume and Intensity: Incorporate high-intensity exercises with an adequate volume to
elicit significant adaptations. Studies suggest programs lasting less than 10
weeks (15 sessions) and high-intensity workouts with over 40 jumps per
session, are most effective (Davies et al., 2015). - Specificity: Tailor exercises to mimic sport-specific movements. For instance, soccer
players may benefit from drills that simulate cutting, pivoting, and rapid
acceleration/deceleration (Buckthorpe & Villa, 2020), and progressively add
caos/unpredictability.
Example Exercises
- Standing Drop jump: landing before jumping. Once the athlete have reaquired landing
capacity, il will be pretty straight forward to progress to jumping - Squat Jumps: Start with bilateral squat jumps, ensuring proper technique and soft
landings. Progress to single-leg squat jumps as strength and control improve - Box Jumps: Begin with low box jumps, focusing on explosive take-offs and controlled
landings. Increase the height of the box and incorporate lateral and rotational
jumps. - Depth Jumps: Use depth jumps to improve eccentric control and reactive strength. Start
with a low drop height and gradually increase as the athlete’s ability allows. - Bounding Drills: Incorporate bounding drills to enhance horizontal power and
coordination. Begin with two-legged bounds and progress to single-leg
bounds.
Table 1: this table, taken from Buckthorpe 2021, shows and summarize most of the aspect
could be useful to create a comprehensive PT program during ACLR rehabilitation of an
athlete.
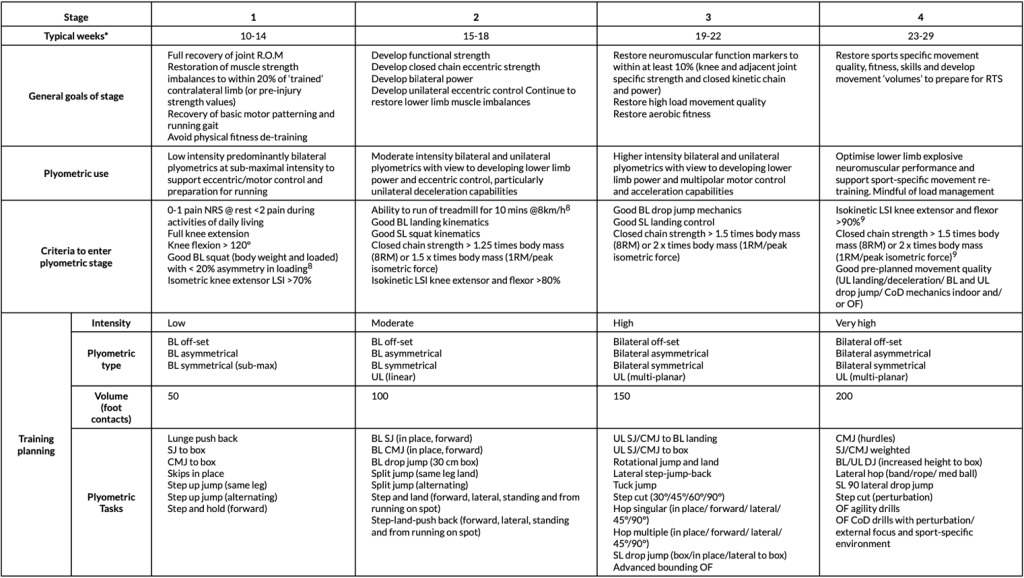

Table 2: This table represents an example of 16 weeks PT with uninjured athletes, that has
been found effective in modifying biomechanical characteristics at the knee level that are
associated with injury risk reduction taken from Bocheng 2024.
| Phase | Exercise | Intensity | Repetitions and Sets |
| 1-4 weeks | Tuck Jump | Medium | 10 × 2 |
| Long Jump | Low | 10 × 2 | |
| 1/4 Squat Jump | Low | 10 × 2 | |
| Box Jump (40cm) | Low | 10 × 2 | |
| Box Jump Down (40 cm) | Medium | 10 × 2 | |
| 5-8 weeks | CM Hurdle Jump | Medium | 6 x 4 |
| Continuous Long Jump | Medium | 6 x 4 | |
| Box Jump without Arm Swing (40cm) | Medium | 6 x 4 | |
| Lateral Box Jump (40cm) | Medium | 6 x 4 | |
| Drop Jump (40cm) | High | 6 x 4 | |
| 9-16 weeks | Lateral Hurdle Jump | Medium | 10 x 2 |
| Depth to Box Jump (40cm) | High | 5 x 4 | |
| Depth to Broad Jump (40cm) | High | 5 x 4 | |
| Lateral Box Jump (40 cm) | High | 5 x 4 | |
| RotaRonal VerRcal Hop | Medium | 10 x 2 |
Monitoring and Feedback
Continuous monitoring and feedback are essential for ensuring proper technique and
progression. Utilize video analysis and feedback to help athletes correct
their form and improve movement efficiency (Buckthorpe & Villa, 2020). No increase in
pain and swelling are warranted (Buckthorpe & della Villa, 2021)
Conclusion
Plyometric training is a crucial, yet often underutilized, component of ACL rehabilitation. Its
benefits in enhancing muscle power, neuromuscular control, and movement quality
make it indispensable for athletes aiming to return to high-level performance. The
introduction of plyometric training should be at an early stage with low intensity
proposals, to ensure that there is time to allow the necessary adaptations to be able
to introduce higher intensity proposals. By following evidence-based guidelines and
incorporating progressive, sport-specific plyometric exercises, strength and
conditioning coaches can significantly improve rehabilitation outcomes and reduce
the risk of re-injury
Bibliography:
Arundale, A. J. H., Bizzini, M., Dix, C., Giordano, A., Kelly, R., Logerstedt, D. S., Mandelbaum, B.,
Scalzi[, D. A., Silvers-Granelli, H., & Snyder-Mackler, L. (2023). Exercise-Based Knee and Anterior
Cruciate Ligament Injury PrevenRon. Journal of Orthopaedic and Sports Physical Therapy, 53(1),
CPG1–CPG34. h:ps://doi.org/10.2519/jospt.2023.0301
Bleakley, C., & Ne:erström-Wedin, F. (2023). Does mechanical loading restore ligament biomechanics
aeer injury? A systemaRc review of studies using animal models. BMC Musculoskeletal Disorders,
24(1). h:ps://doi.org/10.1186/s12891-023-06653-x
Bocheng, C., Ziyan, Y., Jiaxin, W., Wang, G., & Tiancheng, Y. (2024). Effects of 16 weeks of plyometric
training on knee biomechanics during the landing phase in athletes. European Journal of Sport
Science. h:ps://doi.org/10.1002/ejsc.12174
Buckthorpe, M. (2019). OpRmising the Late-Stage RehabilitaRon and Return-to-Sport Training and
TesRng Process Aeer ACL ReconstrucRon. In Sports Medicine (Vol. 49, Issue 7, pp. 1043–1058).
Springer InternaRonal Publishing. h:ps://doi.org/10.1007/s40279-019-01102-z
Buckthorpe, M., & della Villa, F. (2021). RecommendaRons for plyometric training aeer ACL
reconstrucRon – A clinical commentary. InternaBonal Journal of Sports Physical Therapy, 16(3),
879–895. h:ps://doi.org/10.26603/001c.23549
Buckthorpe, M., & Villa, F. Della. (2020). A TEN TASK-BASED PROGRESSION IN REHABILITATION AFTER
ACL RECONSTRUCTION: FROM POST-SURGERY TO RETURN TO PLAY – A CLINICAL COMMENTARY.
InternaBonal Journal of Sports Physical Therapy, 15(4), 611–623.
h:ps://doi.org/10.26603/ijspt20200611
Buckthorpe, M., Villa, F. Della, Villa, S. Della, & Roi, G. S. (2019a). On-field RehabilitaRon Part 1: 4
Pillars of High-Quality On-field RehabilitaRon Are Restoring Movement Quality, Physical
CondiRoning, Restoring Sport-Specific Skills, and Progressively Developing Chronic Training Load.
In Journal of Orthopaedic and Sports Physical Therapy (Vol. 49, Issue 8, pp. 565–569). Movement
Science Media. h:ps://doi.org/10.2519/jospt.2019.8954
Buckthorpe, M., Villa, F. Della, Villa, S. Della, & Roi, G. S. (2019b). On-field RehabilitaRon Part 2: A 5-
stage program for the soccer player focused on linear movements, mulRdirecRonal movements,
soccer-specific skills, soccer-specific movements, and modified pracRce. In Journal of Orthopaedic
and Sports Physical Therapy (Vol. 49, Issue 8, pp. 570–575). Movement Science Media.
h:ps://doi.org/10.2519/jospt.2019.8952
Chmielewski, T. L., George, S. Z., Tillman, S. M., Moser, M. W., Lentz, T. A., Indelicato, P. A., Trumble, T.
N., Shuster, J. J., Cicu[ni, F. M., & Leeuwenburgh, C. (2016). Low- Versus High-Intensity
Plyometric Exercise during RehabilitaRon aeer Anterior Cruciate Ligament ReconstrucRon.
American Journal of Sports Medicine, 44(3), 609–617.
h:ps://doi.org/10.1177/0363546515620583
Davies, G., Riemann, B. L., & Manske, R. (2015). CURRENT CONCEPTS OF PLYOMETRIC EXERCISE. In The
InternaBonal Journal of Sports Physical Therapy | (Vol. 10, Issue 6).
Donaldson, A., Lloyd, D. G., Gabbe, B. J., Cook, J., & Finch, C. F. (2017). We have the Programme, what
next? Planning the implementaRon of an injury prevenRon programme. Injury PrevenBon, 23(4),
273–280. h:ps://doi.org/10.1136/injuryprev-2015-041737
Frobell, R. B., Roos, H. P., Roos, E. M., Roemer, F. W., Ranstam, J., & Lohmander, L. S. (2013). Treatment
for acute anterior cruciate ligament tear: Five year outcome of randomised trial. BMJ (Online),
346(7895). h:ps://doi.org/10.1136/bmj.f232
Grooms, D. R., Palmer, T., Onate, J. A., Myer, G. D., & Grindstaff, T. (2013). Soccer-specific warm-up and
lower extremity injury rates in collegiate male soccer players. Journal of AthleBc Training, 48(6),
782–789. h:ps://doi.org/10.4085/1062-6050-48.4.08
Heidt, R. S., Sweeterman, L. M., Carlonas, R. L., Traub, J. A., & Tekulve, F. X. (2000). Avoidance of Soccer
Injuries with Preseason CondiRoning. In THE AMERICAN JOURNAL OF SPORTS MEDICINE (Vol. 28,
Issue 5).
Herrington, L., Myer, G., & Horsley, I. (2013). Task based rehabilitaRon protocol for elite athletes
following Anterior Cruciate ligament reconstrucRon: A clinical commentary. In Physical Therapy in
Sport (Vol. 14, Issue 4, pp. 188–198). h:ps://doi.org/10.1016/j.ptsp.2013.08.001
Kasmi, S., Zouhal, H., Hammami, R., Clark, C. C. T., Hackney, A. C., Hammami, A., Chtara, M., Chortane,
S. G., Salah, F. Z. Ben, Granacher, U., & Ounis, O. Ben. (2021). The Effects of Eccentric and
Plyometric Training Programs and Their CombinaRon on Stability and the FuncRonal Performance
in the Post-ACL-Surgical RehabilitaRon Period of Elite Female Athletes. FronBers in Physiology, 12.
h:ps://doi.org/10.3389/fphys.2021.688385
Kotsifaki, R., Korakakis, V., King, E., Barbosa, O., Maree, D., Pantouveris, M., Bjerregaard, A., Luomajoki,
J., Wilhelmsen, J., & Whiteley, R. (2023). Aspetar clinical pracRce guideline on rehabilitaRon aeer
anterior cruciate ligament reconstrucRon. BriBsh Journal of Sports Medicine, 57(9), 500–514.
h:ps://doi.org/10.1136/bjsports-2022-106158
Lohmander, L. S., Englund, P. M., Dahl, L. L., & Roos, E. M. (2007). The long-term consequence of
anterior cruciate ligament and meniscus injuries: OsteoarthriRs. In American Journal of Sports
Medicine (Vol. 35, Issue 10, pp. 1756–1769). h:ps://doi.org/10.1177/0363546507307396
Mandelbaum, B. R., Silvers, H. J., Watanabe, D. S., Knarr, J. F., Thomas, S. D., Griffin, L. Y., Kirkendall, D.
T., & Garre:, W. (2005). EffecRveness of a neuromuscular and propriocepRve training program in
prevenRng anterior cruciate ligament injuries in female athletes: 2-Year follow-up. American
Journal of Sports Medicine, 33(7), 1003–1010. h:ps://doi.org/10.1177/0363546504272261
Owoeye, O. B. A., VanderWey, M. J., & Pike, I. (2020). Reducing Injuries in Soccer (Football): an
Umbrella Review of Best Evidence Across the Epidemiological Framework for PrevenRon. In
Sports Medicine – Open (Vol. 6, Issue 1). Springer Science and Business Media Deutschland
GmbH. h:ps://doi.org/10.1186/s40798-020-00274-7
Petushek, E. J., Sugimoto, D., Stoolmiller, M., Smith, G., & Myer, G. D. (2019). Evidence-Based Best-
PracRce Guidelines for PrevenRng Anterior Cruciate Ligament Injuries in Young Female Athletes: A
SystemaRc Review and Meta-analysis. In American Journal of Sports Medicine (Vol. 47, Issue 7,
pp. 1744–1753). SAGE PublicaRons Inc. h:ps://doi.org/10.1177/0363546518782460
Silvers-Granelli, H. J., Bizzini, M., Arundale, A., Mandelbaum, B. R., & Snyder-Mackler, L. (2017). Does
the FIFA 11+ Injury PrevenRon Program Reduce the Incidence of ACL Injury in Male Soccer
Players? Clinical Orthopaedics and Related Research, 475(10), 2447–2455.
h:ps://doi.org/10.1007/s11999-017-5342-5
Steffen, K., Myklebust, G., Olsen, O. E., Holme, I., & Bahr, R. (2008). PrevenRng injuries in female youth
football – A cluster-randomized controlled trial. Scandinavian Journal of Medicine and Science in
Sports, 18(5), 605–614. h:ps://doi.org/10.1111/j.1600-0838.2007.00703.x
Waldén, M., Atroshi, I., Magnusson, H., Wagner, P., & Hägglund, M. (2012). PrevenRon of acute knee
injuries in adolescent female football players: Cluster randomised controlled trial. BMJ (Online),
344(7858). h:ps://doi.org/10.1136/bmj.e3042
Whalan, M., Lovell, R., Steele, J. R., & Sampson, J. A. (2019). Rescheduling Part 2 of the 11+ reduces
injury burden and increases compliance in semi-professional football. Scandinavian Journal of
Medicine and Science in Sports, 29(12), 1941–1951. h:ps://doi.org/10.1111/sms.13532